Science Magazine is one of my favorite publications, mostly for the pictures, and I also enjoy the “Working life” essay which appears at the end of each issue. This week’s Science piece was entitled “Lab meetings shouldn’t feel intimidating. Here’s how I’ve changed mine,” by Georgia Fousteri PhD, a researcher in Milan, Italy. She writes,
At the start of our lab meeting, I did something unconventional: I read my students a poem. “As you set out for Ithaka; hope your road is a long one; full of adventure, full of discovery,” begins “Ithaka” by the Greek poet Constantine Cavafy. Then I asked what the words meant to them.
Imagine that, art being used to kick off a science meeting. Dr Fousteri continues,
I have led a 20-minute team building session at the start of every lab meeting. My lab members and I play parts in inspirational scripts, practice meditation, or do some other activity—including discussing poetry. These sessions have eased tensions and opened minds, helping foster more participation later in the meeting.
What is our hospital and clinic meetings and teaching conferences did the same? This seems like more than team building – it actually has to do with relationship building and personal growth. She continues,
I do not know where this journey with my students will take us. But so far, I feel hopeful about the lab environment we’re creating. My greatest wish is to see my trainees become their best selves, understand who they are and what they want, and reach their career goals. That’s a legacy I can be proud of.
Brilliant. I hope more organizations can include art/music as the number one item on their meeting agendas in 2022.
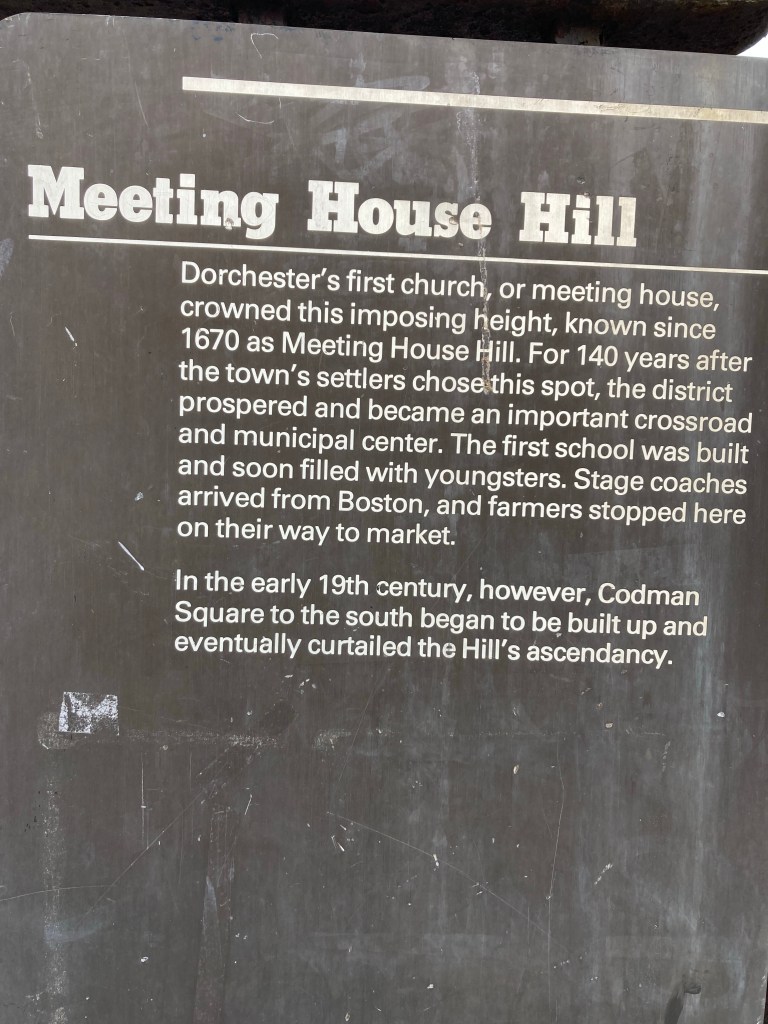
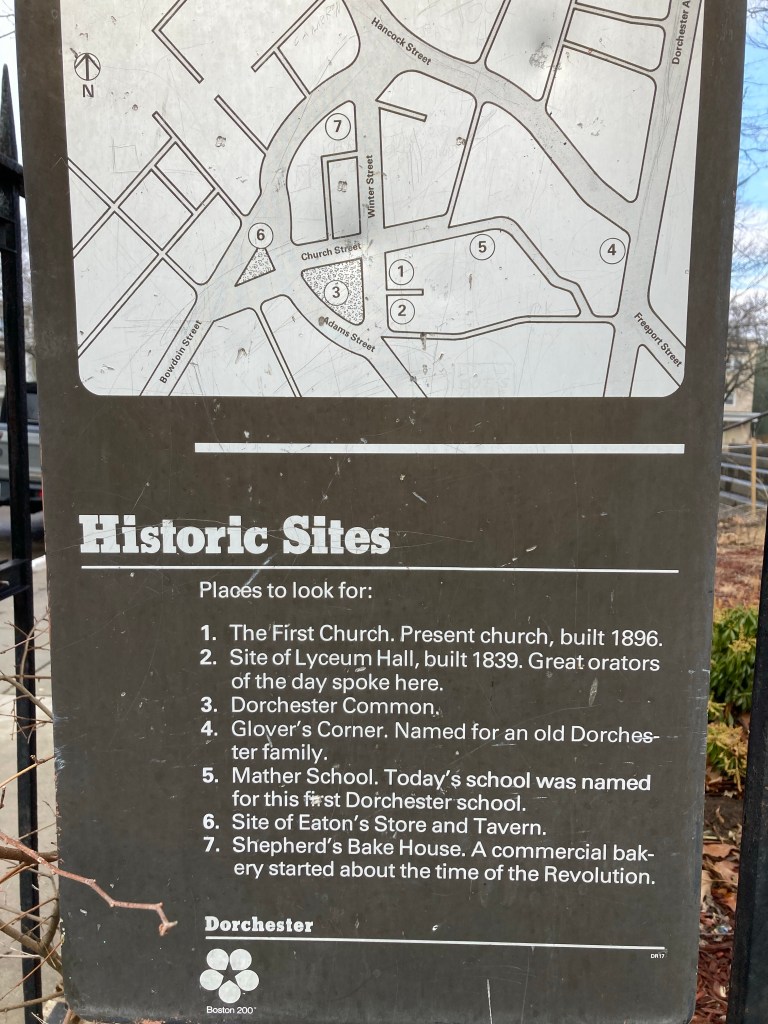
We had our first walking club of 2022 yesterday at Upham’s Corner health center. Check out some photos from our 35 minute stroll around beautiful, historic Dorchester. We even were able to see the ocean! The walking club leaves from the front of the health center every Tuesday at 12:30 PM. We can regain our physical and mental health, together, by walking, and eventually by jogging and running. It’s not too late. Most important is to start slow and walk with other people! You can speed up later on.
First church, 1670Remembering the Covid deadOldest public elementary school!Great mural at the Mather SchoolMusic school next to the health center
Thich Nhat Hanh, the well-known Zen master, died recently in Vietnam at the temple where he lived. An author, poet and teacher, he spoke about “engaged Buddhism,” applying Buddhist principles to social issues and in daily life.
But what does this really mean, and how can people who don’t identify as Buddhists learn from Thich Nhat Hanh’s teaching? Today I want to look at the implications of his work for Health and Healing.
On slowing down
“There is no need to run, strive, search or struggle. Just be. Just being in the moment in this place is the deepest practice of meditation. Most people cannot believe that just walking as if you have nowhere to go is enough.”
What I know best is American medicine, and as a doctor I can say our field is in crisis. It has truly lost its way, between the electronic medical record, lack of time with patients, profiteering, and burnout. Workaholism is the culture of medicine and that is antithetical to Health and Healing. We physicians and other healers need to slow way down. See less patients. Write less emails and Epic notes. Just go for a walk, and listen to the birds.
On death
“Our greatest fear is that when we die we will become nothing. Many of us believe that our entire existence is only a life span beginning the moment we are born or conceived and ending the moment we die. We believe that we are born from nothing and when we die we become nothing. And so we are filled with fear of annihilation.
Doctors, nurses, and other clinicians must address the fear of death over and over. Say a patient has laryngeal tuberculosis. He or she is probably afraid. We absorb that fear, and without healing rituals we are at risk of getting sick ourselves.
On meditation
“Breathing in, repeat, ‘in the here, in the here.’ Breathing out, ‘in the now, in the now.’ Although these are different words, they mean exactly the same thing. I have arrived in the here, I have arrived in the now. I am home in the here. I am home in the now.”
Before we give SSRIs or benzodiazepines for anxiety or depression, we should teach our patients to breathe. To meditate. To be calm. Pills might still be necessary. But they are not a panacea. Hopes and prayers for health and healing, we tell ourselves.
On war
“We know very well that airplanes, guns and bombs cannot remove wrong perceptions. Only loving speech and compassionate listening can help people correct wrong perceptions. But our leaders are not trained in that discipline, and they only rely on the armed forces to remove terrorism.”
Of course the only answer is non-violence. Of course we must stand up for a peaceful, verdant world.
On mindfulness
“With mindfulness, you can establish yourself in the present in order to touch the wonders of life that are available in that moment.”
So to the clinicians out there who are struggling because of COVID, I say to you, be present with your emotions. Validate your pain. And then move on. Organize. Speak out. Sing out. We shall overcome.
On suffering
“We have the tendency to run away from suffering and to look for happiness. But, in fact, if you have not suffered, you have no chance to experience real happiness.”
I have suffered. So have you. Let’s be grateful for our traumas. They help us grow and transform, a metamorphosis.
On fear
“Most of us experience a life full of wonderful moments and difficult moments. But for many of us, even when we are most joyful, there is fear behind our joy… Fearlessness is not only possible, it is the ultimate joy. When you touch nonfear, you are free.”
I agree, of course. If we can identify our greatest fears, understand their root causes, and validate them, even thank them, then we can move on.
Say my greatest fear is developing severe mental illness and being locked up in a psychiatric ward, pumped full of drugs, getting electroconvulsive therapy, and eventually withering up and dying alone. That fear, of psychiatry and psychiatrists, can erode at my happiness and lead to anxiety. But if I can say “thank you” to that fear, that enables me to imagine a better future, and to heal.
On happiness
“There is no way to happiness — happiness is the way.”
The case described the situation of a 57-year-old man with five months of epigastric pain and 15 pound weight loss, HIV/AIDS with a CD4 of 16, and liver masses which had a biopsy demonstrating B-cell lymphoma, for which he was treated with antiretrovirals and chemotherapy.
Four weeks later, he developed sudden bright red blood per rectum, tachycardia, and extravasation in the jejunum from a branch of the superior mesenteric artery. He underwent surgery on his small intestine, and pathology demonstrated acute inflammation of the lamina propria with cytoplasmic and nuclear inclusions surrounded by a clear halo (“owl eye”). Then, he developed blurred vision, and was diagnosed with CMV retinitis and hemorrhagic enteritis. He was treated with oral valganciclovir, IV ganciclovir, and maintenance gancyclovir, as well as chemotherapy, and has gotten much better, with a CD4 count of 337.
I don’t have much of a comment regarding the medical management of the case. My concern is that in 2022 we continue to have patients presenting with advanced HIV/AIDS and CD4 counts of 16. They should be diagnosed much earlier in their course. And ideally, with a variety of preventive methods including PrEP, these HIV infectious should never happen in the first place. But we need a single payer / Medicare-for-all system to fix this “leaky cascade.” We need to rebuild our community health centers and public health infrastructure nationwide – this must be an urgent priority.
Please remember, my blog is completely free. Please leave a comment below if you like! Thanks.
Earlier today, I sat in the fifth row at Boston’s Symphony Hall, next to my seventy-one year old mother, and we watched and listened as the Me/2 Orchestra performed selections by Berlioz, Elgar, Rossini, Grieg, Beethoven, and Milad Yousufi, a young Afghan composer. It was an inspirational, yet odd experience to be in the audience, because I have been an active member of the Me/2 Orchestra for the past several years, playing the violin. I even had the opportunity to join the group on New York City’s Lincoln Center Plaza last October.
But the past couple of months I felt uneasy about Omicron safety measures, and I decided not to participate in rehearsals for the Symphony Hall concert. Even as recently as a week ago I changed my mind and decided to play in the concert, but then flip-flopped again one afternoon when I felt under the weather. However, this is Symphony Hall, home of the Boston Symphony Orchestra, and I had to come see my friends perform.
I’m certainly biased, but I think the music today was beautiful, particularly Freedom, Yousufi’s hypnotic, gyrating work which alternated between G-minor and G-major chords, with E-flat and D thrown in. Concertmaster James Hanford and principal bassist Rusty Chandler led with panache, as inspirational Ronald Braunstein spurred the group on. If you had been worried about the imbroglio of Omicron transmission, like I was, there was no mention of it. During a standing ovation, the young composer Yousufi half-bounded, half-danced his way toward the stage, his long hair bouncing in the air.
Milad Yousufi, composer of Freedom
During the show, I was thinking about how the United States has mistreated Afghanistan over the years, and the current crisis there, a “tsunami of hunger” under American sanctions. But moreover, I was pondering the topic of “mental illness” itself, because the Me/2 Orchestra’s mission is to end stigma regarding mental health through classical music.
Of course, people suffer and become quite distressed (I’ve been there, more than once). They feel nervous, get “the blues,” and sometimes have psychosis, wild ideas, and become impaired. But “depression,” “anxiety,” or “mania” are very different from HIV, tuberculosis, lung cancer, or diabetes.
In HIV, we have a viral load. In tuberculosis we have a PCR as well as Acid Fast Bacilli smear and culture to look for the mycobacterium tuberculosis bacteria. Lung cancer is diagnosed based on biopsy by a well-trained pathologist, and diabetics can measure their blood sugar. In short those four diseases have objective, scientific ways of making a diagnosis and guiding treatment. Their therapies are based on randomized-placebo controlled, blinded clinical trials and meta-analyses.
In comparison, biological psychiatry is mostly an art, even as it often attempts to portray itself as mostly a science. “SIGECAPS,” the acronym used to diagnose depression, is subjective, for example. It’s difficult to be a psychiatrist, because patients often are unhappy, nervous, and can get quite sick, and the American health care system is broken. But importantly, coercion in psychiatry is dangerous, as the late Dr. Thomas Szasz, a Hungarian-American professor explained in his book, “The Myth of Mental Illness.”
Thomas Szasz M.D.
We also need to pay attention to the writing of Erving Goffman, medical sociologist, who wrote Asylums. Moreover, what we need to do is understand the root causes of mental sickness, from genetics to adverse childhood experiences to trauma and social factors. Medical anthropology as a discipline can play a key role here, and I feel fortunate to have worked closely with a medical anthropologist in Mozambique in 2013 and to have absorbed a bit about the discipline.
In addition, we need to learn more about the recovery process, particularly how tools like Wellness Recovery Action Plans can help. A mental health “diagnosis” like “depression” is not necessarily a lifelong one.
Another big issue is something called the “sick role” – as elaborated by medical sociologist Talcott Parsons in 1951. I believe the passivity of the sick role can be overcome for many people, through a focus on wellness-promoting activities, such as music, dancing, and exercise.
Me/2 Orchestra warming up before today’s concert
I’m not saying I’m against all psychiatric medications – I am a licensed, practicing physician who takes pills prescribed to me, after all. But everyone knows that pills are not a panacea.
In any event, music can help end the stigma and discrimination regarding mental health, if each of us speaks out. And the Me/2 Orchestra certainly put on a badass show at Symphony Hall this afternoon. Here’s to more works by Milad Yousufi, action to end the starvation in Afghanistan, and to healing in 2022!
I recently enrolled in Colin Turner’s excellent twelve week running course here in Boston. Colin, a former college track and cross country star at College of Wooster, brings an infectious, positive attitude to his teaching. Our cohort of students are learning about everything from exercise physiology to running gear, and study technique of elite marathoners such as Eliud Kipchoge. Colin has us take videos of ourselves running, so we can analyze our form, and he has an emphasis on staying healthy and avoiding running injuries.
This is not a part of Colin’s course, but one thing I’ve always been interested in is barefoot running. (Of course winter in Boston is not a good time to try it). But it makes sense from an evolutionary perspective – because 20,000 years ago, when we were hunter gatherers, chasing down wild game, certainly we weren’t wearing Nikes.
Therefore, I took a brief look at a 2019 scientific paper by Karsten Hollander et al from Germany which investigates barefoot running. The reason for conducting such a study is that whether running barefoot is beneficial for running performance and injury risk has is quite controversial. No clear evidence has been provided yet to answer this question.
Previous studies showed that changing acutely from wearing shoes to barefoot running induces several changes to running biomechanics. These adaptations include changing from a rearfoot to more anterior foot strike pattern (midfoot or forefoot strike) as well as reduced foot and ankle dorsiflexion at ground contact.
In this study, the German researchers reported that a habituation to barefoot running led to increased vertical average loading rates. Their finding was quite unexpected and questions the generalizability of acute adaptations to long-term barefoot running. The bottom line is more research is needed regarding barefoot running versus wearing shoes, and the debate remains wide open.
I like the idea of occasional barefoot running in the summer when the ground is warm, provided you can find a path to jog on with no glass or other sharp objects that can hurt to feet. Running or walking barefoot really connects you to nature.
What do you think? Have you ever jogged barefoot outside? Please leave a comment below.
Eliud Kipchoge, the world’s best marathoner, certainly wears shoes when he runs a 1:59 marathon.
In medicine, we are often focused on sickness and disease rather than wellness and prevention. How much time in medical school do we spend learning about HIV, syphilis, gonorrhea, and chlamydia for example, rather than the biopsychosocial and cultural aspects of sexual health? I know medical school isn’t about training anthropologists, but the social sciences are important.
Let me back up. Sexuality is about reproduction, so we must think about evolutionary biology. But it is also about culture. In a culture where violence is praised, women and LGBTQ+ people are often the victims of sexual violence.
So we must start from the beginning, from birth, modeling healthy communication in our families, and we must not tolerate sexual violence in any form.
Couples therapy and family therapy should be much more available and less stigmatized. Healthy sexual relationships throughout the lifespan should be our priority.
In the clinic, we need time to talk to patients regarding sexual health, who their partners are, and prevention of sexually transmitted infections. This can be the difference between life and death, in the case of taking PrEP to prevent HIV transmission, for example.
But time is what we don’t have in the clinic. The norm is the 15-30 minute visit. So we are rushing, and having a discussion about sexuality takes time.
We also need much people in sexual relationships to listen to each other much better. When a partner says no,, that means no. But it also brings up an important question – why is s/he saying no? What are our emotions, and why do we have them? I am not going to go too much farther there, because doing so would require a discussion of Sigmund Freud and Jacques Lacan, but these are important topics.
When I graduated from the University of Pennsylvania School of Medicine in 2008, there was no SARS Cov-2 virus. We still treated hepatitis C with pegylated interferon and ribavirin. We didn’t have the glp-1 agonists like dulaglutide to treat diabetes, or continuous glucose monitoring devices.
Medicine is constantly changing, and clinicians struggle to stay up-to-date in our knowledge base. We read medical journals and UpToDate, but is that enough? Primary care review courses, like the Harvard one led by David W. Bates, MD, MSc, Jane S. Sillman, MD, and Cristina B. Alexander, MD are available, but they are costly.
So here’s my question – what is the best way to “sharpen the saw” – is it a traditional CME course? And what about board certification, for those of us who trained in internal medicine or family medicine? Do those certification exams reflect the reality of outpatient medical practice in 2022?
I wish CME courses were clearly pharma-free, affordable, and relevant. They should be customizable- for example I have developed an interest in pain management, ultrasound, and the musculoskeletal physical exam since I started my new job at Upham’s Corner Health Center nine months ago. Those topics, along with nutrition, exercise counseling, opioids, and motivational interviewing, are key CME topics for outpatient primary care.
Primary care is exciting, even thrilling. It’s great to practice preventive medicine and get to know families over time in a neighborhood. We need a single payer/ Medicare for all, and improved electronic medical record, to attract clinicians to federally qualified community heath centers. We can do it, if we organize and Imagine – think of the song by John Lennon.
I stood in front of the Massachusetts State House yesterday, a sunny, windy Martin Luther King Jr day. The state police officers had returned to their vehicle and I breathed deeply, then started reading the names of the COVID dead once more.
Martha stood next to me, a brave family physician trained in the Montefiore residency system, where my mentor Dr Charlie Van Der Horst also trained back in the 1970s. Susan, a primary care internist here in Boston working hard to provide excellent medical care to patients in America’s broken health care system, was on my right, looking off into the distance.
Millions dead from COVID, and the deaths continue to mount. I read the names, one by one. Some names were hard to pronounce, others easier. And then I froze. James Hakim, Zimbabwe.
Dr Hakim is dead? From COVID? I had no idea! Terrible.
I never met Dr Hakim personally, but I heard a about him back in 2011 – 2012, when I was in Mozambique working on the Medical Education Partnership Initiative. Dr Hakim was a legendary South Sudanese – Ugandan physician scientist and leader in the HIV field. Along with others such as Eric Goosby, Chip Schooley, Connie Benson, Fitzhugh Mullen, and Emilia Noormahomed, Dr Hakim was trying to ensure that the physician workforce crisis in Sub-Saharan Africa improved. Residency programs, medical schools, and research infrastructure were being established. It was a hopeful time, despite HIV/AIDS and so many other crises in the region.
We have lost so much during this COVID pandemic.
We must bear witness to our losses, if we are to regain our hope.
In 1963, my aunt, Mary Ann Lederer, and my father, Albert, traveled from Cincinnati to Washington DC to attend the March on Washington for Jobs and Freedom. Together, they heard Dr. Martin Luther King Jr’s famous speech, “I have a Dream.”
Then in 1965, in the wake of “Bloody Sunday” on the Edmund Pettus Bridge, Dr. King called for volunteers to come down to Alabama to assist during the March from Selma to Montgomery. My father drove down with a friend, and volunteered at the Dexter Avenue Baptist Church. At the conclusion of the march, Dr. King gave a speech at the Alabama State House, and then came over to Dexter. He shook the hands of many of the volunteers, including my fathers’.
Well here we are in 2022. Things are different, but they are the same. In Boston, a small group of us are planning a silent vigil today outside the Massachusetts State House, for Health and Healing, despite the ugly winter weather. We agree with the Dalai Lama that the most radical thing people can do is come together and listen to each other, with compassion. That’s what Dr. King did. That’s what Mahatma Gandhi did. That’s what Nelson Mandela did. And that’s what my father did, until he died suddenly of a heart attack in October 2020.
–
There is far too much vitriol in our society. We must stop this political polarization. Take the case of two women, Boston Mayor Michelle Wu, and CDC Director Rochelle Walensky. I have spoken to Mayor Wu a couple of times, and know Dr. Walensky personally, and I am dismayed by the way they are treated by the general public and in the mainstream media. That’s not to say that I don’t disagree with many of their policies. I do. But I think there is a lot of misogyny going on here and that is very dangerous. The previously elected Boston Mayor, Marty Walsh, never received the kind of hateful treatment that Mayor Wu is getting. And previous CDC Directors Thomas Frieden and Robert Redfield never had to deal with the kind of abuse Dr. Walensky is facing. But it goes beyond misogyny. Mayor Wu is facing anti-Asian bigotry and Dr. Walensky is having to deal with anti-Semitism.
So today, figure out a way to advocate for the marginalized, the poor, the undocumented immigrants, the sick, the children. You don’t have to come out with us in the rain at the Massachusetts State House at 12 PM, although you are certainly welcome to do so.